Overview
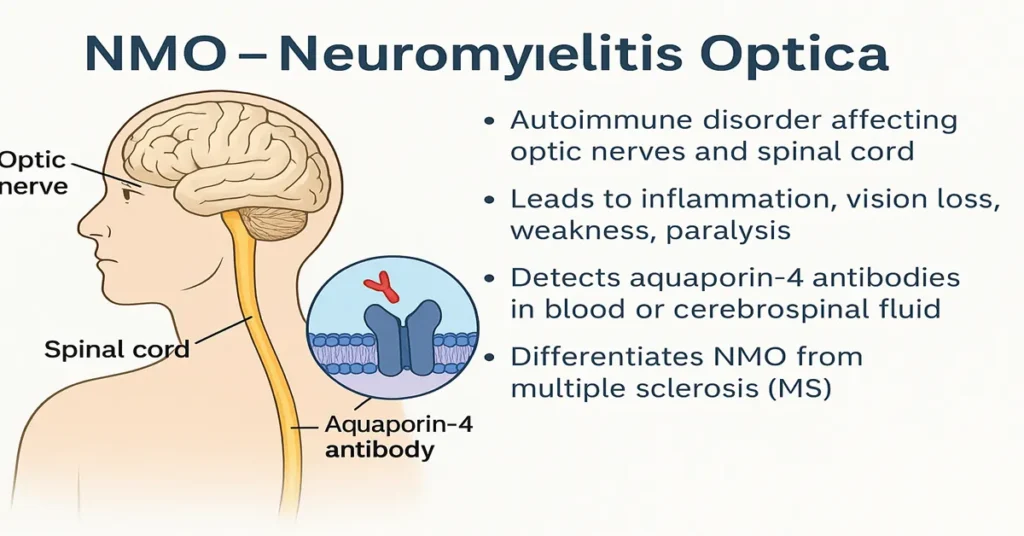
Neuromyelitis Optica (NMO), also known as Devic’s disease, is a rare but serious autoimmune disorder that primarily affects the optic nerves and spinal cord. In this condition, the body’s immune system mistakenly attacks components of the central nervous system, leading to inflammation and damage of nerve tissue. Because early symptoms of NMO can resemble those of multiple sclerosis (MS), accurate testing and timely diagnosis are essential to reduce the risk of long-term neurological disability.
NMO is characterized by episodes of optic neuritis and transverse myelitis. These episodes may result in vision impairment, weakness, sensory changes, or bladder and bowel difficulties. In some cases, symptoms can be severe. Understanding the disease process and the role of the AQP4 (Aquaporin-4) Antibody Test is central to identifying the condition correctly and guiding further care.
What Exactly Is NMO?
Neuromyelitis Optica is an autoimmune neurological condition in which the immune system produces antibodies that target aquaporin-4 water channels. These channels are found on astrocytes, which are supportive cells in the brain and spinal cord. Damage to these channels leads to inflammation and disruption of normal nerve signaling, particularly in the optic nerves and spinal cord.
NMO typically follows a relapsing course, meaning symptoms appear in distinct attacks. Each episode has the potential to cause lasting nerve damage, which is why early recognition and diagnosis are especially important from a clinical perspective.
Difference Between NMO and Multiple Sclerosis (MS)
Although NMO and MS may initially appear similar, they are distinct conditions with important differences.
MS often involves multiple areas of the brain, while NMO primarily affects the optic nerves and spinal cord. The immune mechanisms underlying the two disorders are different, and treatments effective for MS may be ineffective or even harmful in NMO. The presence of AQP4 antibodies is a key distinguishing feature, as these antibodies are associated with NMO and not with MS. Additionally, attacks in NMO tend to be more severe and may result in greater residual disability.
For these reasons, laboratory testing and careful clinical assessment are critical to ensure the correct diagnosis.
Where Are NMO-Related Antibodies Produced?
NMO itself is not produced by the body; rather, it is a disease state resulting from immune dysfunction. The antibodies involved in NMO, known as AQP4-IgG antibodies, are produced by B-lymphocytes, a type of immune cell.
These antibodies mistakenly recognize aquaporin-4 channels as harmful. Once they bind to these channels on astrocytes, they trigger inflammation and tissue injury within the optic nerves and spinal cord. This immune-mediated process explains the neurological symptoms observed in affected patients.
Importance of the NMO (AQP4 Antibody) Test
The AQP4 Antibody Test plays a central role in diagnosing Neuromyelitis Optica and guiding further evaluation.
Confirming the Diagnosis
A positive AQP4 antibody result strongly supports a diagnosis of NMO and helps distinguish it from MS and other neurological disorders.
Guiding Treatment Decisions
Because treatment approaches differ significantly between NMO and MS, confirming the correct diagnosis is essential to avoid inappropriate therapies.
Preventing Disability
Early identification allows clinicians to initiate appropriate medical strategies aimed at reducing inflammation and lowering the risk of relapse-related nerve damage.
Monitoring Disease Activity
In selected cases, antibody testing may contribute additional information when assessing disease course alongside clinical findings.
Causes of Low / Negative Levels
A negative AQP4 antibody test means that these antibodies were not detected in the sample. However, a negative result does not completely exclude NMO.
Possible explanations include seronegative NMO, testing during early stages of the disease when antibody levels are low, or suppression of antibody levels due to recent treatment. In some cases, symptoms may be due to other conditions such as MS or MOG antibody–associated disease. Further evaluation using imaging studies and additional laboratory tests may be required.
Symptoms of Low / Negative Results
Low or negative antibody results do not cause symptoms themselves. They simply indicate that AQP4 antibodies were not identified at the time of testing.
If neurological symptoms persist despite a negative test, clinicians may consider additional investigations, including testing for other antibodies, MRI studies, or cerebrospinal fluid analysis.
Causes of High / Positive Antibody Levels
A positive AQP4 antibody test reflects the presence of antibodies associated with NMO. This finding suggests an autoimmune process targeting aquaporin-4 channels.
While the exact trigger is not always clear, contributing factors may include immune dysregulation, genetic susceptibility, environmental influences, or the presence of other autoimmune conditions.
Symptoms of High / Positive Levels
When AQP4 antibodies are present, patients may experience symptoms typical of NMO.
Optic Neuritis
This may include eye pain, blurred or reduced vision, difficulty with color perception, or partial to complete vision loss.
Transverse Myelitis
Inflammation of the spinal cord can cause weakness, sensory loss, numbness, tingling, or difficulties with bladder and bowel control.
Brainstem Symptoms
Some patients may experience persistent hiccups, nausea, vomiting, or breathing-related difficulties.
Without appropriate medical care, repeated inflammatory episodes can lead to lasting neurological impairment.
Reference Range
The AQP4 antibody test is generally reported in qualitative terms.
Negative: AQP4 antibodies not detected
Positive: AQP4 antibodies detected
Some laboratories may provide numerical values, but clinical interpretation relies primarily on whether antibodies are present or absent.
Sample Type
The test is most commonly performed using a blood (serum) sample. In certain situations, cerebrospinal fluid may be tested, particularly when blood results are negative but clinical suspicion remains high. CSF analysis can provide additional diagnostic clarity in selected cases.
Diagnosis Process for NMO
Diagnosis of NMO involves a combination of clinical evaluation and laboratory testing. This typically includes a detailed symptom history, AQP4 antibody testing, MRI imaging of the brain and spinal cord, and, when needed, cerebrospinal fluid analysis. Differentiation from MS, MOG-associated disorders, and infections is an essential part of this process.
Early and accurate diagnosis is key to reducing the impact of future relapses.
Treatment Overview (Brief)
Although treatment details are beyond the scope of this test overview, management generally focuses on controlling immune activity and reducing inflammation. Medical care is directed by specialists and tailored to the individual patient’s condition.
Test Preparation
No fasting is required for the AQP4 antibody test. Patients should inform their doctor about current medications, especially immunosuppressive drugs, and any history of autoimmune or neurological conditions. If a lumbar puncture is planned, short-term rest afterward may be advised.
When to Consult a Doctor
Medical attention should be sought if symptoms such as sudden vision changes, eye pain, limb weakness, numbness, difficulty walking, or loss of bladder or bowel control occur. Persistent vomiting, hiccups, or rapidly worsening neurological symptoms also warrant prompt evaluation.
Early consultation supports timely diagnosis and helps reduce the risk of permanent nerve damage.
Important Word Explanations
- Autoimmune: A condition in which the immune system attacks the body’s own tissues
- Optic Neuritis: Inflammation of the optic nerve affecting vision
- Transverse Myelitis: Inflammation of the spinal cord impacting movement and sensation
- Aquaporin-4: A water channel protein involved in NMO
- AQP4-IgG: The antibody associated with Neuromyelitis Optica
- Astrocytes: Supportive cells in the brain and spinal cord
- MRI: Imaging test used to examine the brain and spinal cord
~END~
Related Posts
None found